

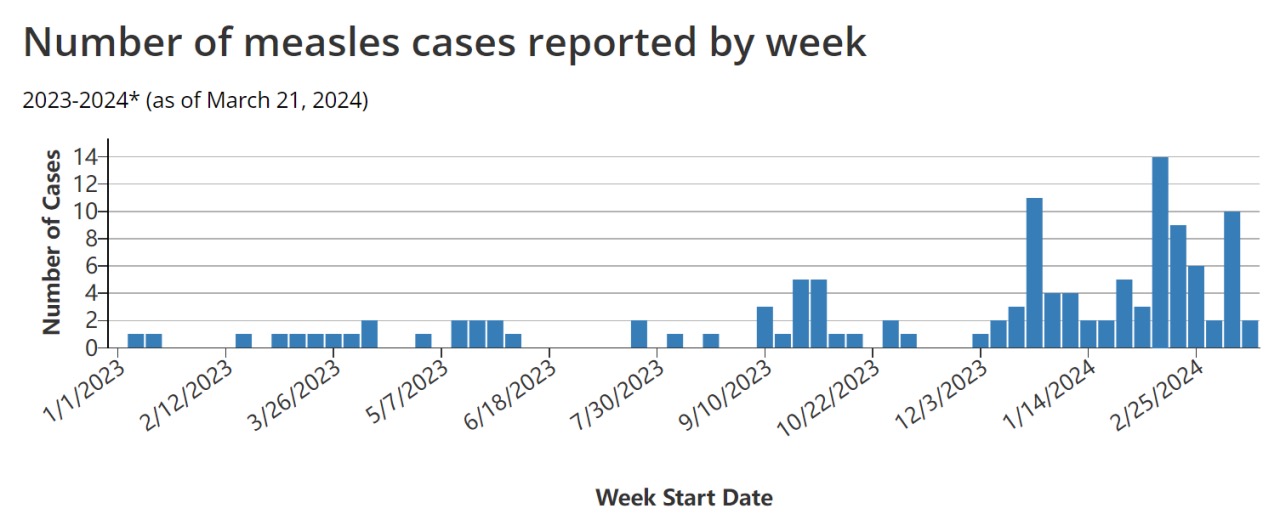
No longer eliminated, measle cases rise during post-COVID period
Measles is caused by the measles virus, a single-stranded negative-sense enveloped RNA virus of the genus Morbillivirus in the family Paramyxoviridae. It is a highly contagious infectious disease that can be prevented through vaccination. Measles typically occurs in unvaccinated or under-vaccinated individuals, who may contract and spread the disease, especially when traveling internationally, to those who are unvaccinated or not immune to measles. The recent increase in imported measles cases reflects the global rise in measles cases and the escalating threat of this dangerous pathogen worldwide.
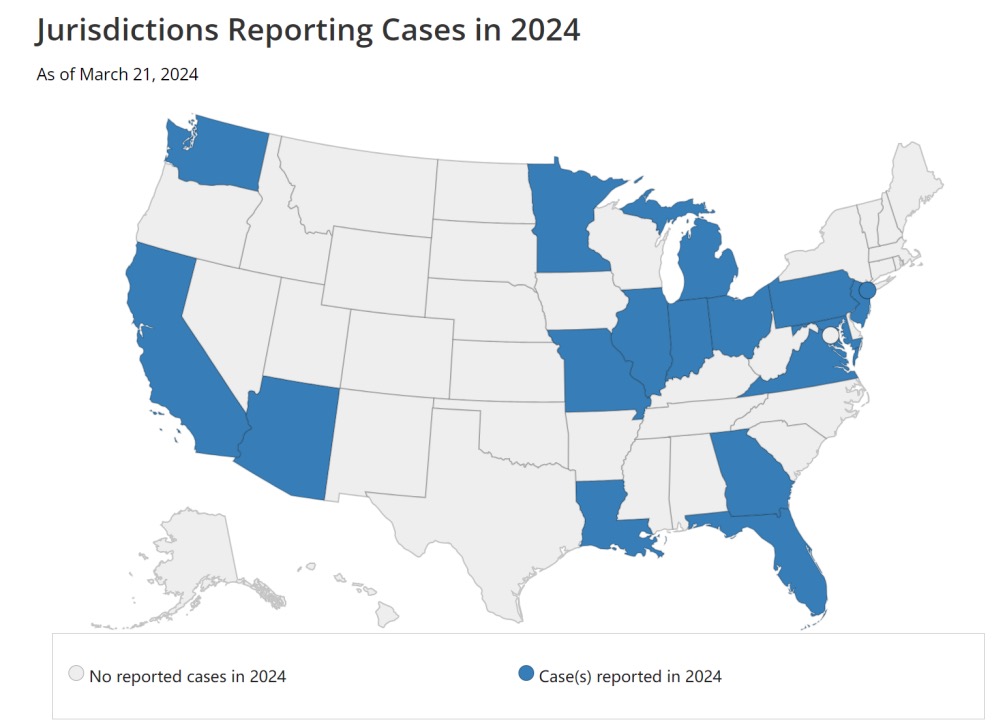
The U.S. government declared measles eliminated in 2000, meaning the disease was no longer endemic in the country. However, if the current measles outbreak persists for a year or longer, the United States may lose its measles elimination status. Doctors cite several factors contributing to measles transmission, with global measles cases on the rise in recent years.
Many of the cases reported in the U.S. this year are associated with international travel, as outbreaks have occurred in destinations such as the United Kingdom, Austria, and the Philippines. In the U.S., many of the infected individuals are children aged 12 months and older who have not received the vaccine. Routine childhood vaccinations, including two doses to prevent measles, mumps, and rubella, were halted after the outbreak began. State-mandated vaccination rates in U.S. kindergartens decreased from approximately 95% in the 2019-20 school year to about 93% in the 2022-23 school year.
Barriers to vaccine access may also contribute to the increase in measles cases in the United States. Experts note that some parents may not be aware that they can get their children vaccinated for free through private insurance or children’s vaccine programs.
While measles can be diagnosed based on typical signs and symptoms, particularly by observing Koplik’s spots, the CDC and other experts strongly recommend laboratory confirmation. Currently, laboratory testing for measles includes collecting nasopharyngeal or throat swab, urine, or blood samples from patients with clinical features of measles. Nasopharyngeal or throat swabs are preferred over urine specimens.
Laboratory diagnosis of measles can be achieved by confirming positive measles IgM antibodies or by detecting measles virus RNA in throat, nasal, or urine samples using RT-PCR. RT-PCR is particularly useful for confirming uncertain IgM antibody results. Saliva can also be used for saliva measles-specific IgA testing, which is sometimes useful for those who cannot provide blood samples. However, saliva-based IgA methods are not preferred due to the presence of many other fluids and proteins in saliva, and the antibody content in saliva is also 1/800 of that in blood samples, which may make sample collection and measles antibody testing difficult.


